

Heart sounds auscultation is a key part of cardiovascular examination, allowing clinicians to assess cardiac function and detect abnormalities such as valve disease, heart failure, or congenital defects. 
Normal Heart Sounds: S1+S2+0 (or ‘lub, dub’)
1. S1 (“Lub”) – First Heart Sound:
Cause: Closure of the mitral (M1) and tricuspid (T1) valves.
Timing: Marks the beginning of systole.
Best heard at: Apex (5th intercostal space, midclavicular line).
Characteristics:
Louder than S2 at the apex.
Normally a single sound, though can be split if M1 and T1 are slightly asynchronous.
2. S2 (“Dub”) – second heart sound:
Cause: Closure of the aortic (A2) and pulmonic (P2) valves.
Timing: Marks the end of systole and beginning of diastole.
Best heard at: Base of the heart (2nd intercostal space, right and left sternal borders).
Splitting:
Physiologic split: A2 before P2 during inspiration (due to delayed RV emptying).
Wide split: Seen in right bundle branch block or pulmonary stenosis.
Fixed split: Seen in atrial septal defect.
Paradoxical split: P2 before A2 (seen in left bundle branch block, aortic stenosis).
Additional Heart Sounds:
3. S3 (Ventricular gallop)
Cause: Rapid ventricular filling into a dilated ventricle.
Timing: Early diastole, just after S2.
Best heard at: Apex (left lateral decubitus position).
Low-pitched, use bell of stethoscope.
Clinical significance:
Normal in children, athletes, pregnancy.
Pathologic in adults — indicates heart failure or volume overload.
4. S4 (Atrial gallop):
Cause: Atrial contraction against a stiff ventricle (↓ compliance).
Timing: Late diastole, just before S1.
Best heard at: Apex (left lateral decubitus).
Low-pitched, use bell.
Clinical significance:
Seen in hypertension, aortic stenosis, hypertrophic cardiomyopathy.
Absent in atrial fibrillation (no atrial contraction).
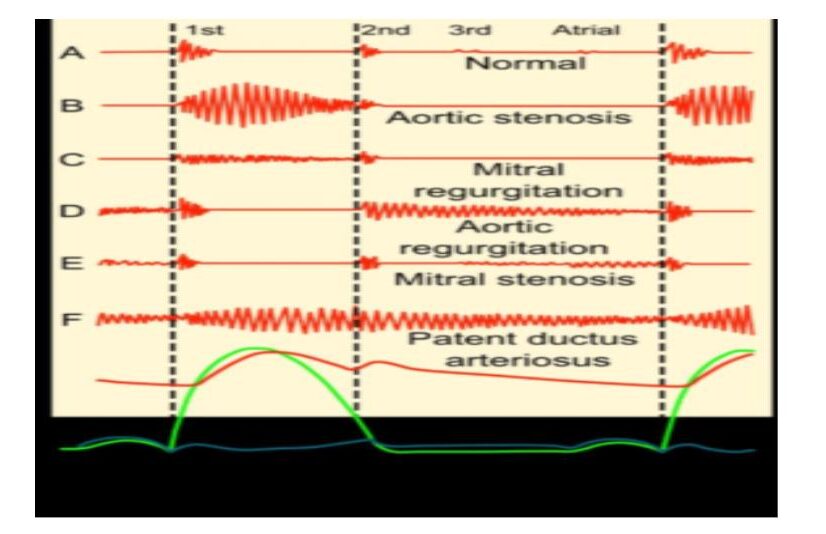
Murmurs
Murmurs are caused by turbulent blood flow, often due to valvular stenosis or regurgitation.
Key Locations for Auscultation: 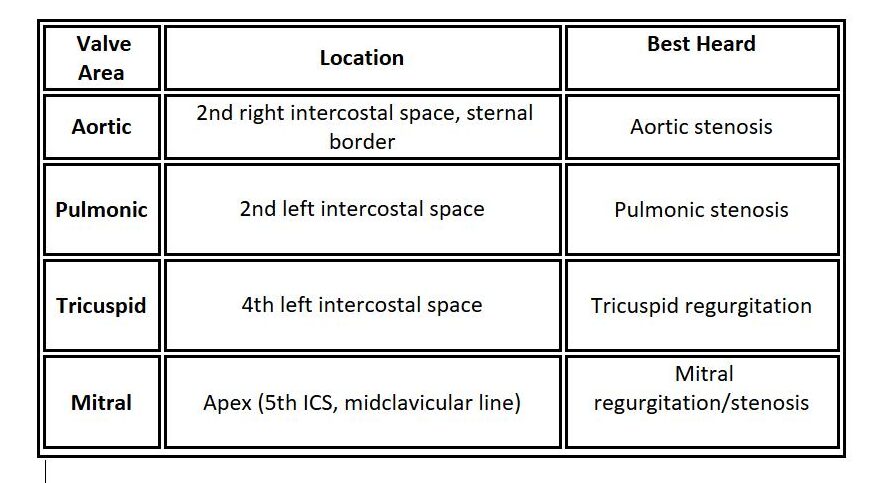
Murmur Timing:
Systolic murmurs: Aortic stenosis, mitral regurgitation.
Diastolic murmurs: Aortic regurgitation, mitral stenosis.
Auscultation Tips:
Use diaphragm (wide part of stethoscope):
For high-pitched sounds (S1, S2, aortic regurgitation, mitral regurgitation).
Use bell (small side of stethoscope):
For low-pitched sounds (S3, S4, mitral stenosis).
Patient positions:
Sitting forward, exhaling: Best for aortic regurgitation.
Left lateral decubitus: Best for mitral stenosis and S3/S4.
Listen in all 4 valve areas systematically — use both bell and diaphragm.
Auscultation Positions (Valve Areas):
These correspond to where each valve’s sound is best heard, not where the valve actually lies. 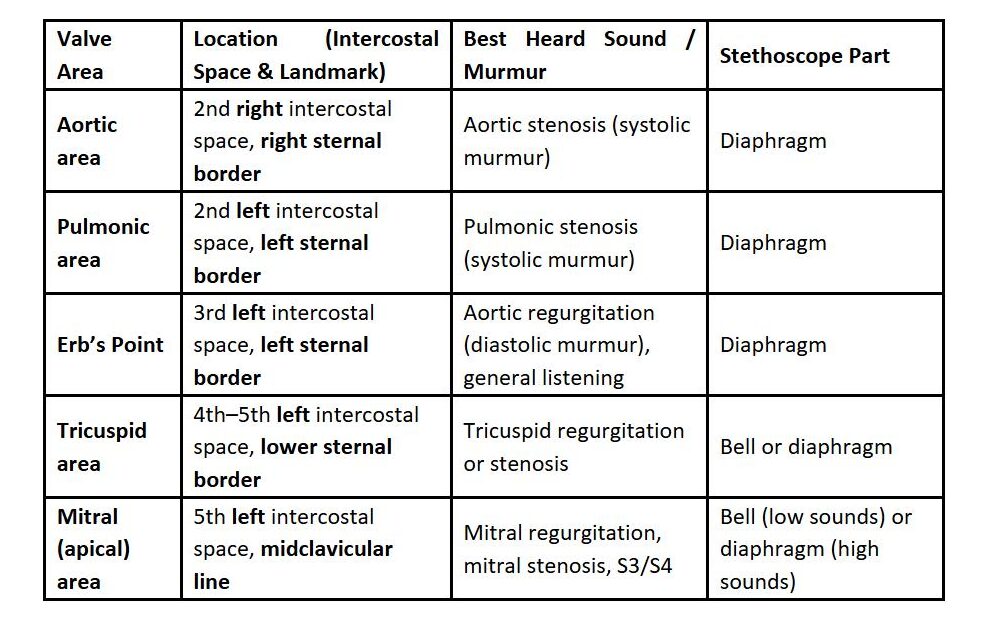
Simple Diagram Summary
Here’s how the stethoscope positions are laid out on the chest (imagine the patient facing you): 
Go Back
